Award Holder: Bryn Trevelyan James
University: University of Manchester
Title of Research: ‘The Healer’s Tools – A Study of Material Assemblages amongst Traditional Practitioners in Ghana and their Archaeological Implications

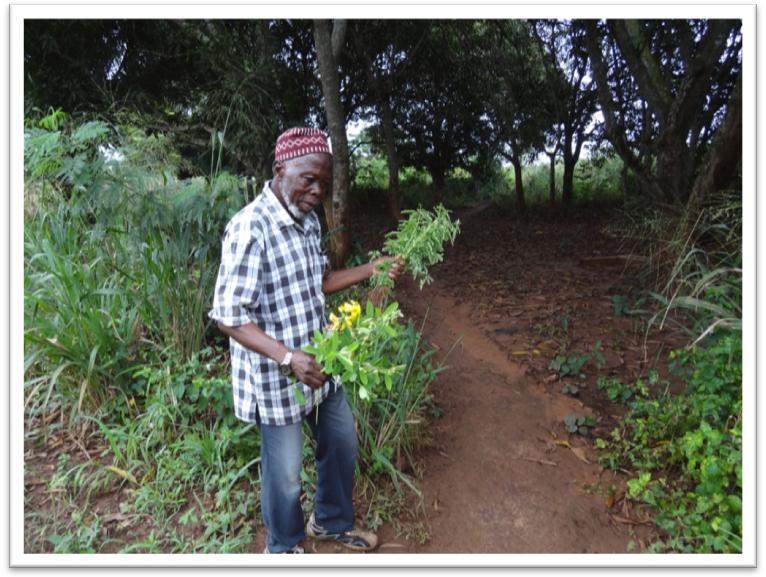
This report concerns two seasons of ethnographic engagement with indigenous medicine practitioners living amongst the migrant population of Madina, a district in Accra, the capital of Ghana. Historically, the importance of itinerant healers across West Africa, living in zongo (strangers’ quarters) communities like Madina has long been recognised (Kobo 2010:71). Problematically, contextualisation of the material dimension of their healing activities, such as the tools of their trade and specific formulations of remedies, is frequently limited (Konadu 2007:1-7). My research sought to expand understandings of these aspects of the healers’ role: exploring the way therapeutic practices shape, and are shaped by, their lived spaces; the artefact assemblages structuring and supporting these practices; and the substances and medicines through which they communicate well-being to others (see Fig. 1). As an archaeologist by training, such contemporary encounters presented me with an opportunity to broaden my perspectives on the kind of interpretive issues to think about when considering evidence of the search for healing in the past.
Work with may-magane (medicine men) in the field led me to first question and then challenge dominant scholarly traditions which present indigenous healing as merely modes of psychotherapy or processes for maintaining social relationships (Csordas & Lewton 1998:436). The richness of participants’ appreciation concerning curative properties of substances in their environments was such that reducing whole bodies of local knowledge to simply imagined panacea seemed dismissive and unrepresentative. I correspondingly began to consider the way in which the role of the healer in active cross-cultural therapeutic relations had been diminished by discourses on African medicine which often exemplify either derogatory or romanticised versions of the traditional healer as fundamentally a static agent (Rekdal 1999:459). Both interpretations rely upon the assumption that indigenous specialists are intrinsically isolated conservatives whose curative methods are limited to dwindling ancestral knowledge (Janzen & Greene 2003:1). My findings suggested that in Madina at least this was not the case, and indeed through observing and aiding practitioners in the preparation of remedies for their clients a more complex picture developed of healers as dynamic and creative.
In response, my methodology, which evolved throughout the project, sought to avoid an abstract question led interview-style of data gathering that would have privileged my preconceptions. Instead I encouraged far more open discussion pathways, which allowed practitioners to tell the stories they wanted to, whilst orientating conversations around themes such as lafiya (wellbeing), spirituality, or particular objects related to the context of the day’s activities. In order to develop the necessary level of trust and establish comfortable relationships participant observation and involvement in daily tasks, like the gathering and processing of herbs, was a prominent feature of the first fieldwork season approach. This allowed me to maintain a patient and respectful presence which served to reassure healers and their dependents of the genuine interest motivating research. In Ghana, where the shadow of past colonialism is still felt and a recent increase in fraudulent behaviour has led to a level of distrust, a sensitive attitude to discussing medicinal knowledge, generally regarded as a family trade secret, proved the most conducive route to openness.
The benefits of carefully building rapport went beyond the surprising levels of personal disclosure offered by healers; it also led to further introductions with more reserved practitioners typically disinclined to talk about their work. Islamic mallams (learned men) pointed me towards secretive underground shrine keepers, market women took me to their Vodu priests and a small-scale domestic healer acted as gatekeeper to Baba Yahaya, the area’s most powerful witchfinder. Although a range of established methodologies were used to systematically expand the contributor base, including the Participant Rapid Appraisal (PRA) approach and snowball-sampling, overall I felt the project developed organically, guided by the informants. Planning and background reading provided the seed for my ideas, the Madina community the soil in which it grew, but it was the participants who offered nourishment and encouragement so that each in their own way should be credited for shaping the different branches of research which developed.

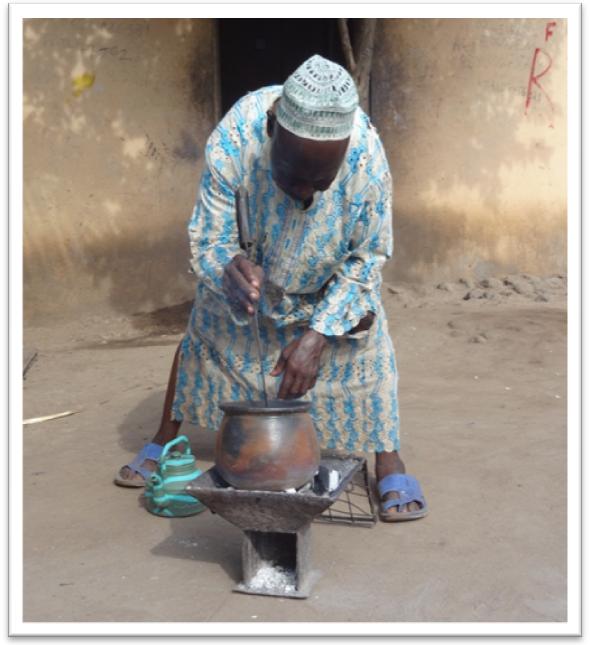
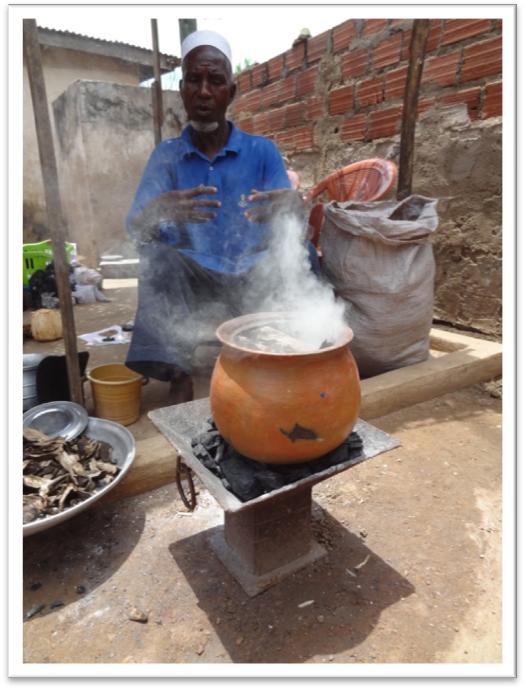
Of course, working within a migrant community that was ethnically, linguistically and religiously diverse was not without its difficulties and challenges. I quickly realised that there could be no talk of a homogenous medical system in the conventional sense. Rather, the different forms of healer, and varied expectations of clients, existed within a mosaic of overlapping, merging fields of practice in which it was impossible, indeed impractical, to attempt to separate the natural from the spiritual, the mundane from the religious. May-magane (medicine men) such as Omar (see Fig. 3), who dealt primarily with substance-based medicines taught me that each plant has a spirit, and that identifying a particular species means little if you cannot follow the rituals and prohibitions that the spirit of the plant dictates. Similarly, encounters with may-jinya (spirit men) deepened my conception of the links between substances and the supernatural: the tangible elements practitioners utilise to mediate between the visible world of man and the invisible world of al-jene (local spirits). This latter form of medicine, combining plants, minerals, animal parts and products with the powers of numinous forces, was contrasted by the orthodox Islamic practices of learned mallams. These Muslim holymen, like Mallam Baki, relied for their cures primarily upon the Quran, the word of Allah. Their medicines were literary-based: the production of layoyi, calligraphic charms containing a portion of Quranic verse, or of rubutu, drinking medicine in which the Word of God literally enters the client’s body (see Fig. 2). However, by observing the work of individual practitioners over time it became clear that the techniques associated with each specialist were in fact often combined. The herbalists strengthened their remedies with prayer, the spiritualist may-jinya were also experts in plant cures for natural ailments like malaria, and behind closed doors respected Islamic mallams performed rituals with al-jene to produce dangerous sambo (bad medicine).
Compared to the task of comprehensively engaging with such a heterogeneous, pluralistic urban medical culture the typical difficulties of fieldwork seem, in hindsight, minor. Bureaucracy, inevitable periods of sickness, the anxiety of making new connections and reaching out to strangers for their help, all become part of the background when you wake up each morning having dreamt of the interview notes typed the night before and sit down to begin planning the day ahead. In this sense, the overarching aims of the project serve to drive one on: there is only ever so much time and with every engagement further possibilities present themselves for exploration. Discourse with the culturally other constantly presents its own set of challenges, particularly, I found, when dealing with a subject as emotive as healing. From a Western perspective the shift in cosmological outlook may be considered jarring, as theories of disease causation, treatment and prevention were often markedly different to the paradigms of scientific medicine. However, having read widely on West African healing and spirituality prior to beginning the project, and benefiting from previous research with elder African community members living in the UK, I had an awareness of magane (medicine) which allowed me to discuss sensitive issues delicately. It also meant I was able to mentally fill in unspoken silences on topics such as sambo (bad medicine) when healers were only comfortable sharing knowledge, or exposing themselves to criticism, up to a certain point.
Conveying an engaging sense of a fieldwork project concerning heterogeneity in a mixed medical system, from which practitioners offer a diversity of healing based upon varied cosmological outlooks, risks confusion. However, by tracing connections through a few ethnographic encounters I hope to offer some insight into my journey as a researcher, which was often stimulated by contradictions in local discourses on wellbeing and that often took me to the vibrant markets looking for answers or examples of some rare material mentioned by a participant.
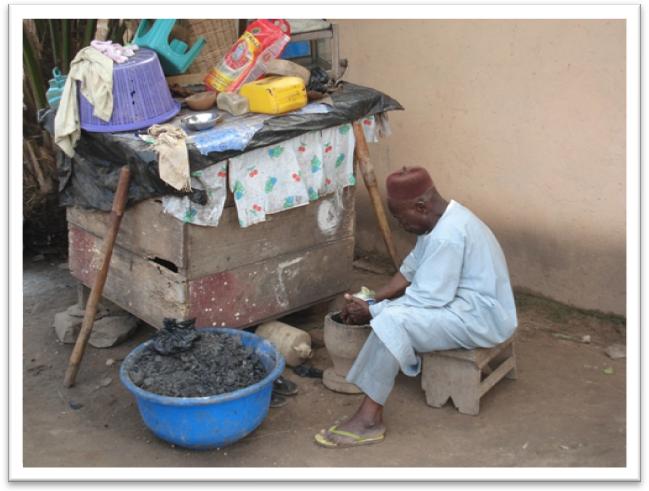
One such exotic substance came into my possession after visiting Baba Yahaya, a man who controlled and was, in turn, controlled by al-jene (see Fig. 4 & 7). Late in the evening I remember him carefully handing me a few jealously guarded strands of what he described as spirit hair. This transference was accompanied by a warning that their owners may seek to take them back. Upon returning to my lodgings that night the hairs were locked away with other specimens collected throughout the afternoon. I went to sleep, only to wake in the morning with a fever and a laptop which refused to start. Needless to say the days planned activities were rescheduled so I could visit Baba again and ensure the al-jene were placated. Sometime later Baba incorporated one of the hairs into a charm known as a laya which I find myself carrying even now. Laya are protective devices, but the accompanying rituals also unspokenly serve to bind the holder to the creator. It is through such experiences that I, as a researcher, felt my conceptions surrounding the materiality of healing transform, from a mundane appreciation of form and purpose, to something more culturally appropriate. In this case, beliefs were catalysed and became performed actions: so I moved implicitly and explicitly towards accepting the numinous conceptions so strongly underlying indigenous dialogues on wellbeing.
Interestingly though, whilst the religious basis necessary for healing serious ailments was acknowledged by all, there was frequently disagreement as to the most suitable focuses of prayer and solicitation. Although the majority of participants were Muslims, some felt local deities were more efficacious for particular problems, whilst others strictly condemned those who would claim any power than that of Allah. The cousins Yussif and Ali exemplified this dichotomy perfectly and nothing embodied these tensions more clearly than a medicine of theirs called the tonnikari, or ‘writing stone’. Consisting of a large smooth white stone collected from the edge of the sea, upon its surface would be written Quranic verse relevant to the client’s problem. The inscribed stone was then boiled in water, which the patient later used to wash with and drink, cleansing them. Yussif insisted that the true power of the medicine came from the water spirits associated with the stone, whilst Ali indignantly ascribed its strength to the Word of God alone. Both agreed, however, that the medicine could only work properly because of this very combination. Such harmonising contradictions threaded their way through much of the project, and identifying where, and perhaps why, distinct traditions had been woven together into new forms became a central emphasis of the research.
Nowhere was the complexity of mixed migrant healing traditions more clearly expressed than in the wares of female traders at the medicine suppliers section of the Timber Market. The largest site of its kind in Ghana, it was here healers came for rare and exotic substances: dried barks and roots from across West Africa, endangered animals smuggled into the country, esoteric objects such as Ewe Vodu dolls and metal fetishes essential for religious rites. Sitting in the shade of a stall at the market you are surrounded not only by the materiality of healing, but encounter all the different actors sustaining indigenous medicine as a vibrant tradition, for here they come to buy and sell, seek advice, and pass the time. Healers from Madina introduced me to the market women, including Mrs Mother (see Fig. 5), but it was primarily through the market that I came to know people whose activities provided the raw resources for local therapeutics: the herb gatherers and animal trappers, drum makers and figure carvers, peddlers of cure-alls and well-dressed body snatchers. Indeed the market could be considered both a metaphor and microcosm encapsulating African urban healing more generally: diverse, adaptable, at times ambiguous but always accessible to those seeking resolution. The wares at each stall express a need for healing derived from both the natural power of plants and mediation with the supernatural: a space in which tradition and innovation co-exist and the exotic or the other consistently find a welcome. Surprisingly, the Timber Market has yet to be the subject of in-depth anthropological investigation, thus presenting an exciting direction for future research.

Turning to think about the practical implications of my work up to this point, I would hope that at a local level the findings may inform aspects of planning among health-related NGOs active in Madina and similar communities. These groups already offer support and accreditation to herbalists, however my experiences suggest it would be beneficial if this was extended more widely, including practitioners typically overlooked on the basis that they are concerned with spiritual matters only. The mallam and the may-jinya all possess a basis of herbal and physiological knowledge which if supplemented by additional training and official recognition (that many felt excluded from) could lead to additional health benefits, especially amongst migrant communities where presenting therapies in a culturally appropriate manner is essential.
In a broader sense, and specific to my project aims, the outcomes of the research have a wide range of implications for indicating possible alternative interpretations and sources of evidence for healing in the past. Techniques and beliefs associated with the acquisition, preparation and application of medicines closely documented in the field add contextual depth to consideration of comparable processes in the archaeological record (e.g. Insoll 2007, 2011a; van Dongen, Fraser & Insoll 2011). At the same time, the collection and description of a wide range of objects and materials associated with indigenous healing traditions presents an opportunity to contribute to understandings of often poorly provenanced ethnographic assemblages held at institutions across the country.
Currently I am working on a number of articles distilling different research themes touched upon here and through these runs the argument that indigenous healing ought to be understood as a dynamic, living cultural expression. Studying the herbal and spiritual medicines of Madina reveals healers, on the one hand, to be creative agents, adapting elements from distinct practices to produce syncretic therapies which objectively unify competing Islamic and indigenous systems. At the same time the may-magane are repositories and keepers of knowledge carefully transmitted as an inheritance between generations. From an archaeological perspective then, the contemporary ‘traditional’ West African practitioner is at once an active, professional craftsperson, a source of dynamism and change, and also a guide to the past, capable of offering an interpretive window on residues of activities they identify as their own. The concluding word on this dual role of the traditional healer is perhaps best left to Chief Adamu Zakaria (see Fig. 6):
“What is the may-magane? I am the potter and the pot. I am the legs and the head of the magane. From me new medicines proceed, and in me the medicines of my father are stored.”
Bibliography
Csordas, T. J. & Elizabeth Lewton, E. (1998) Practice, performance and experience in ritual healing. Transcultural Psychiatry 35: 435-512
Insoll, T. (2007) ‘Natural’ or ‘human’ spaces? Tallensi sacred groves and shrines and their potential implications for aspects of Northern European prehistory and phenomenological interpretation. Norwegian Archaeological Review 40, 2: 138-158.
Insoll, T. (2011) Substance and materiality? The archaeology of Talensi medicine shrines and medicinal practices. Anthropology and Medicine 18, 2: 181-203.
Janzen, J.M. & Green, E.C. (2003) Continuity, change, and challenge in African medicine, (in) Selin, H. (ed.) Medicine across cultures: History and the practice of medicine in Non-Western cultures. London: Kluwer Academic Publishers. 1-26.
Kobo, O. (2010) ‘We are citizens too’: the politics of citizenship in independent Ghana. The Journal of Modern African Studies 48: 67-94.
Konadu, K. (2007) Indigenous Medicine and Knowledge in African Society. London: Routledge.
Rekdal, O.B. (1999) Cross-cultural healing in East African ethnography. Medical Anthropology Quarterly 13, 4: 458-482.
Van Dongen, B.E., Fraser, S.E. & Insoll, T. (2011) The composition and origin of Ghana medicine clays. Anthropology and Medicine 18, 2:285-302.